
SARS-CoV-2 Prevalence on and Incidence after Arrival in Travelers on Direct Flights from Cape Town, South Africa to Munich, Germany Shortly after Occurrence of the Omicron Variant in November/December 2021: Results from the OMTRAIR Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Procedures
2.3. Primary Outcomes
2.4. Information from Questionnaire
2.5. Statistical Analysis
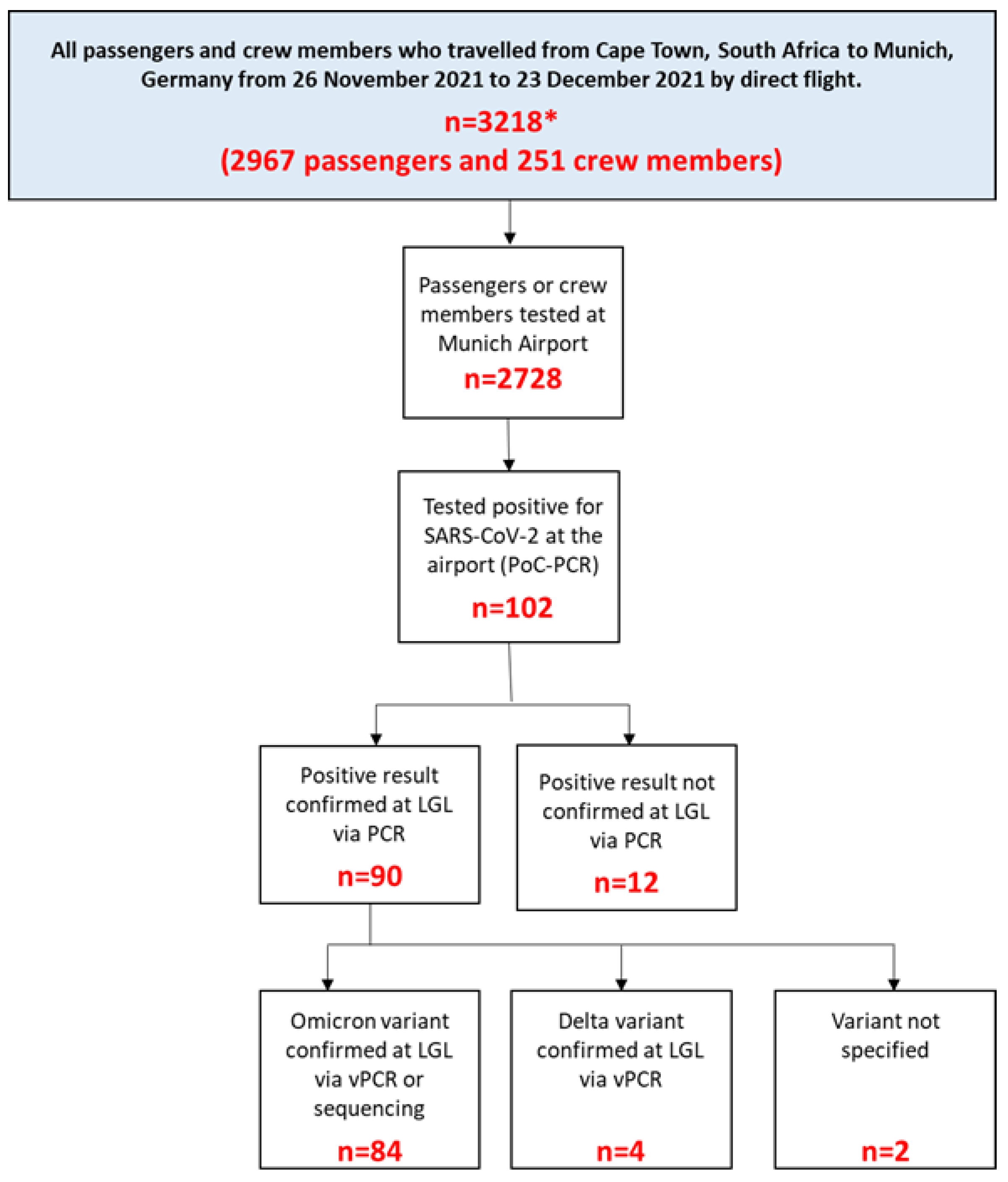
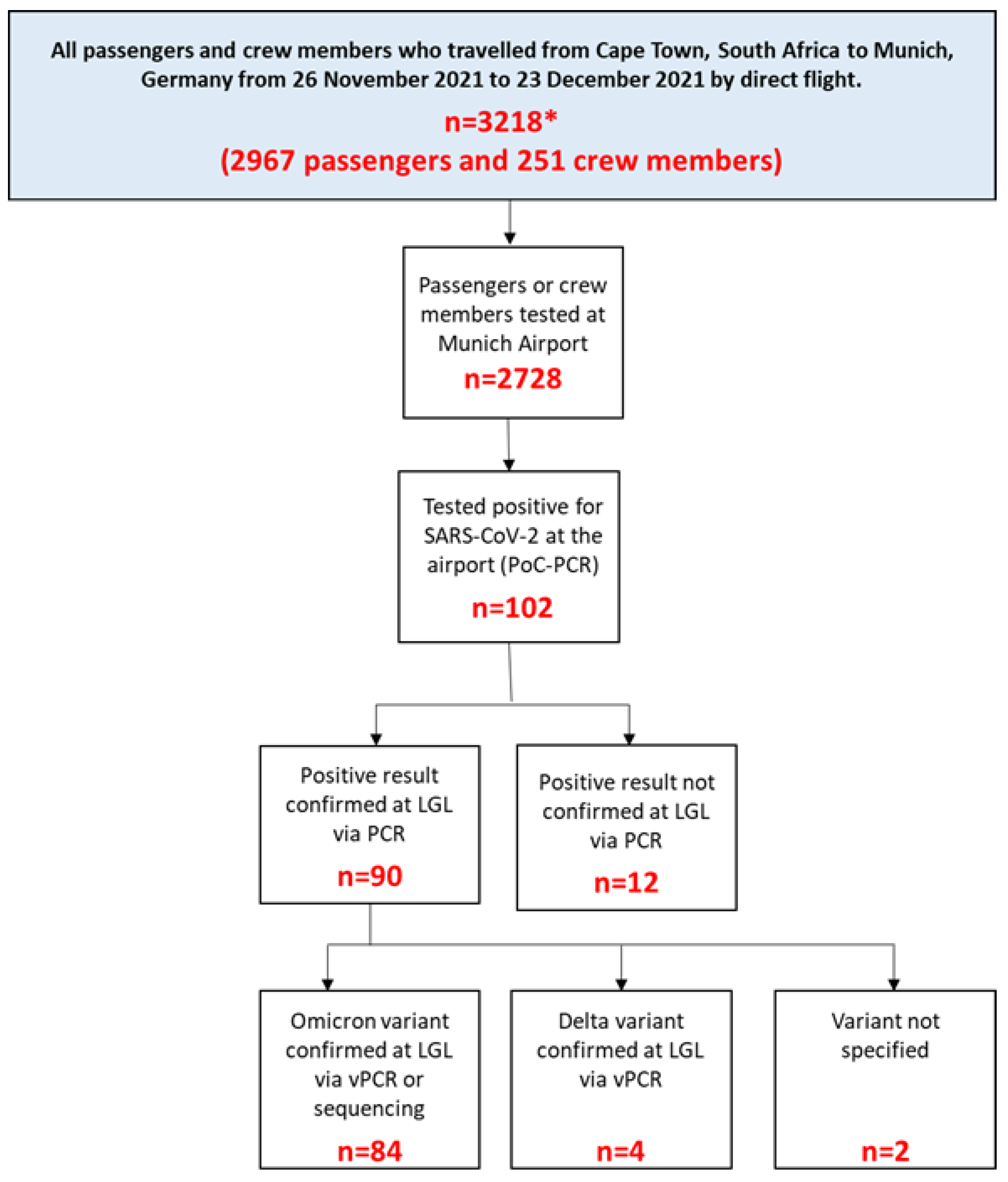
3. Results
3.1. SARS-CoV-2 Prevalence on Arrival
3.2. SARS-CoV-2 Incidence within 14 Days after Arrival among Study Participants
3.3. Symptoms
3.4. Compliance with Entry Regulations and Prevention Measures
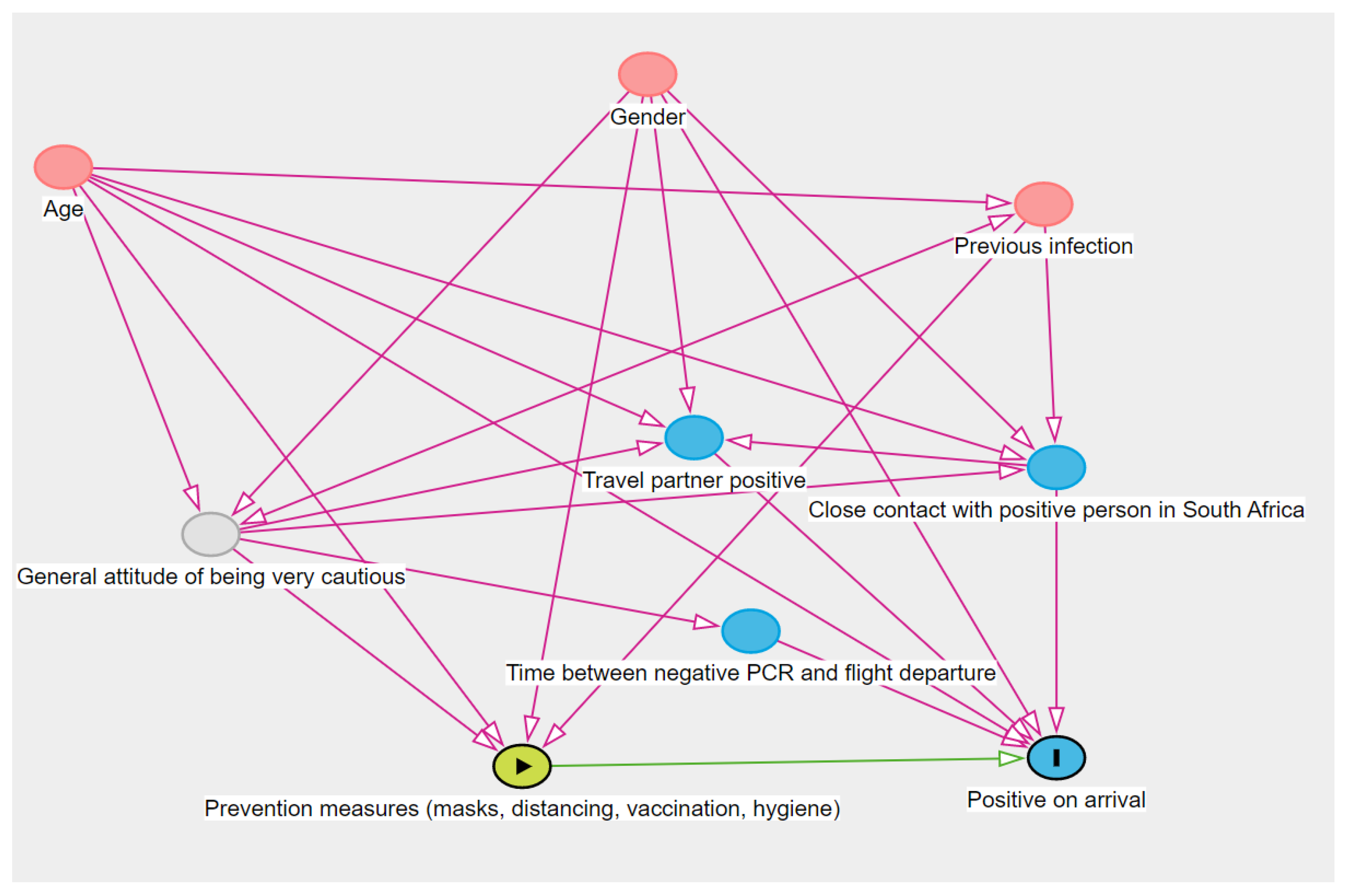
3.5. Associations with Testing Positive on Arrival
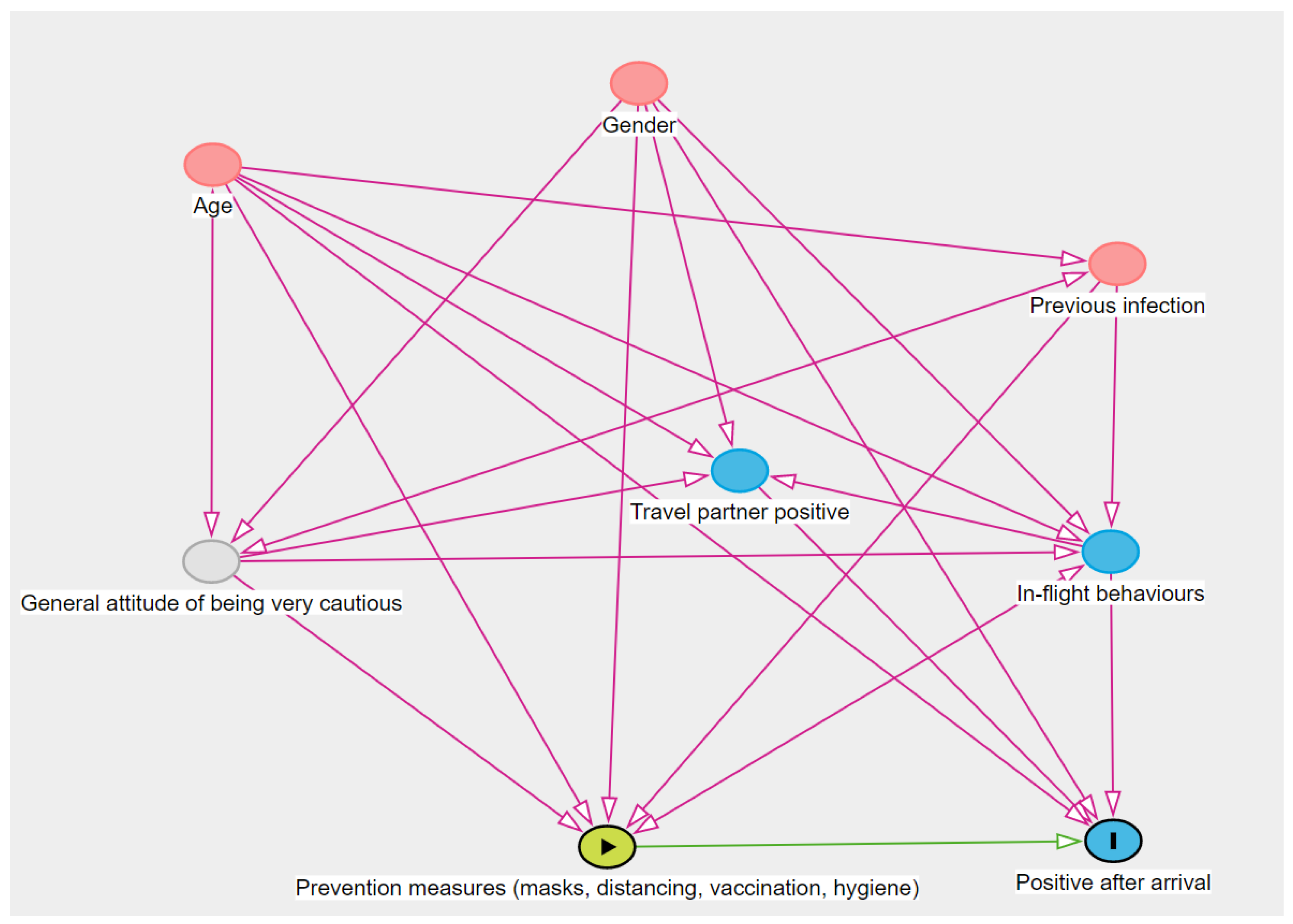
3.6. Associations with Incident Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date of Flight | Tested for SARS-CoV-2 on Arrival at Munich Airport | Tested Positive for SARS-CoV-2 on Arrival at Munich Airport and Confirmed at the LGL Laboratory |
|---|---|---|
| N = 2728 (100%) | N = 90 (3.3%) | |
| 26 November 2021 | 237 (100%) | 2 (0.84%) |
| 28 November 2021 | 305 (100%) | 15 (4.91%) |
| 1 December 2021 | 262 (100%) | 8 (3.05%) |
| 3 December 2021 | 251 (100%) | 11 (4.38%) |
| 4 December 2021 | 260 (100%) | 5 (1.92%) |
| 5 December 2021 | 203 (100%) | 5 (2.46%) |
| 6 December 2021 | 199 (100%) | 5 (2.51%) |
| 8 December 2021 | 230 (100%) | 6 (2.61%) |
| 10 December 2021 | 155 (100%) | 9 (5.81%) |
| 11 December 2021 | 97 (100%) | 4 (4.12%) |
| 12 December 2021 | 101 (100%) | 5 (4.95%) |
| 13 December 2021 | 48 (100%) | 2 (4.17%) |
| 15 December 2021 | 87 (100%) | 3 (3.45%) |
| 17 December 2021 | 73 (100%) | 6 (8.22%) |
| 18 December 2021 | 52 (100%) | 0 (0%) |
| 19 December 2021 | 54 (100%) | 2 (3.70%) |
| 20 December 2021 | 41 (100%) | 2 (4.88%) |
| 22 December 2021 | 46 (100%) | 0 (0%) |
| 23 December 2021 | 27 (100%) | 0 (0%) |
| Symptoms | Total |
|---|---|
| N = 28 (100%) | |
| Fever (≥38.0 °C/100.4°F) | 4 (16%) |
| Cough | 18 (67%) |
| Rhinitis, sneezing | 15 (54%) |
| Chest pain | 3 (12%) |
| Headache | 23 (82%) |
| Skin rash | 1 (4%) |
| Fatigue or exhaustion | 21 (81%) |
| Chills | 8 (32%) |
| Shortness of breath | 8 (32%) |
| Sore throat | 16 (62%) |
| Decrease or loss of smell or taste | 2 (8%) |
| Pain in limbs | 10 (40%) |
| Diarrhoea | 5 (20%) |
| Nausea, vomiting, abdominal pain | 2 (8%) |
| Conjunctivitis | 1 (4%) |
| Swelling of lymph nodes | 3 (12%) |
| Hospitalized | 0 (0%) |
| Potential Confounders, Added One by One to Each Exposure Model | |||||||
|---|---|---|---|---|---|---|---|
| Exposures | Age | Gender | Positive Travel Partner | Close Contact | Prevention Measures (Just Sign. Ones) | Previous SARS-CoV-2 Infection (Not Significant) | Time between Test and Departure |
| Reporting a positive travel partner | No change | No change | N/A | No change | Avoided mass transportation: unable to run; Rest: no change | No change | RR decreased by 13% (less sign.) RR = 2.63, 95%CI = 0.97–6.19, p = 0.037 |
| Wore mask indoors and outdoors | No change | No change | No change | No change | N/A | No change | No change |
| Avoided mass transportation | No change | No change | Unable to run | RR + 11% (more sign.) RR = 5.12, 95%CI = 1.46–19, p = 0.010 | N/A | No change | RR + 27% RR = 5.86, 95%CI = 1.42–28, p = 0.013 |
| Avoided contact with people outside my travel group | No change | No change | No change | No change | N/A | No change | RR + 12% (not sign. anymore) RR = 3.88, 95%CI = 0.99–26, p = 0.083 |
| Potential Confounders, Added One by One to Each Exposure Model | |||||
|---|---|---|---|---|---|
| Exposures | Age | Gender | In-Flight Behaviors (Not Evaluated Because All Were Not Associated with the Outcome) | Prevention Measures (Not Evaluated Because All Were Not Associated with the Outcome) | Previous SARS-CoV-2 Infection (Not Significant) |
| Age 1 | N/A | RR + 20% (not sign. anymore) RR = 0.48, 95%CI = 0.21–1.15, p = 0.086 | N/A | N/A | No change |
| Gender 1 | RR—11% (but still sign.) RR = 3.16, 95%CI = 1.25–9.59, p = 0.024 | N/A | N/A | N/A | No change |
| Reporting a positive travel partner | No change | No change | N/A | N/A | No change |
References
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. 26 November 2021. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 12 December 2022).
- World Health Organization. Tracking SARS-CoV-2 Variants 2022. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 12 December 2022).
- European Center for Disease Prevention and Control. Threat Assessment Brief: Implications of the Emergence and Spread of the SARS-CoV-2 B.1.1. 529 Variant of Concern (Omicron) for the EU/EEA 2021. 26 November 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/threat-assessment-brief-emergence-sars-cov-2-variant-b.1.1.529 (accessed on 12 December 2022).
- European Center for Disease Prevention and Control. Weekly Epidemiological Update: Omicron Variant of Concern (VOC)—Week 1 (Data as of 7 January 2022) EU/EEA 2021. Available online: https://www.ecdc.europa.eu/en/news-events/weekly-epidemiological-update-omicron-variant-concern-voc-week-1-data-7-january-2022 (accessed on 12 December 2022).
- Liu, Y.; Rocklöv, J. The effective reproductive number of the Omicron variant of SARS-CoV-2 is several times relative to Delta. J. Travel Med. 2022, 29, taac037. [Google Scholar] [CrossRef] [PubMed]
- Daon, Y.; Thompson, R.N.; Obolski, U. Estimating COVID-19 outbreak risk through air travel. J. Travel Med. 2020, 27, taaa093. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.; Bambury, N.; Boland, M. In-flight transmission of wild-type SARS-CoV-2 and the outbreak potential of imported clusters of COVID-19: A review of published evidence. Glob. Health 2021, 17, 93. [Google Scholar] [CrossRef] [PubMed]
- Khanh, N.C.; Thai, P.Q.; Quach, H.-L.; Thi, N.-A.H.; Dinh, P.C.; Duong, T.N.; Mai, M.T.Q.; Nghia, N.D.; Tu, T.A.; Quang, L.N.; et al. Transmission of SARS-CoV 2 During Long-Haul Flight. Emerg. Infect. Dis. J. 2020, 26, 2617. [Google Scholar] [CrossRef]
- Blomquist, P.B.; Bolt, H.; Packer, S.; Schaefer, U.; Platt, S.; Dabrera, G.; Gobin, M.; Oliver, I. Risk of symptomatic COVID-19 due to aircraft transmission: A retrospective cohort study of contact-traced flights during England’s containment phase. Influ. Other Respir. Viruses 2021, 15, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Jansen, L.; Tegomoh, B.; Lange, K.; Showalter, K.; Figliomeni, J.; Abdalhamid, B.; Iwen, P.C.; Fauver, J.; Buss, B.; Donahue, M. Investigation of a SARS-CoV-2 B.1.1.529 (Omicron) Variant Cluster—Nebraska, November-December 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1782–1784. [Google Scholar] [CrossRef]
- Tanaka, H.; Ogata, T.; Shibata, T.; Nagai, H.; Takahashi, Y.; Kinoshita, M.; Matsubayashi, K.; Hattori, S.; Taniguchi, C. Shorter Incubation Period among COVID-19 Cases with the BA.1 Omicron Variant. Int. J. Environ. Res. Public Health 2022, 19, 6330. [Google Scholar] [CrossRef]
- Bielecki, M.; Patel, D.; Hinkelbein, J.; Komorowski, M.; Kester, J.; Ebrahim, S.; Rodriguez-Morales, A.J.; Memish, Z.A.; Schlagenhauf, P. Air travel and COVID-19 prevention in the pandemic and peri-pandemic period: A narrative review. Travel Med. Infect. Dis. 2021, 39, 101915. [Google Scholar] [CrossRef]
- Tande, A.J.; Binnicker, M.J.; Ting, H.H.; Del Rio, C.; Jalil, L.; Brawner, M.; Carter, P.W.; Toomey, K.; Shah, N.D.; Berbari, E.F. SARS-CoV-2 Testing Before International Airline Travel, December 2020 to May 2021. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2021; Volume 96, pp. 2856–2860. [Google Scholar]
- Choi, E.M.; Chu, D.K.W.; Cheng, P.K.C.; Tsang, D.N.C.; Peiris, M.; Bausch, D.G.; Poon, L.L.M.; Watson-Jones, D. In-Flight Transmission of SARS-CoV-2. Emerg. Infect. Dis. 2020, 26, 2713–2716. [Google Scholar] [CrossRef]
- Freedman, D.O.; Wilder-Smith, A. In-flight transmission of SARS-CoV-2: A review of the attack rates and available data on the efficacy of face masks. J. Travel Med. 2020, 27, taaa178. [Google Scholar] [CrossRef]
- Richter, D. Bayerns Erste Omikron-Fälle im Landkreis München-Umsichtiges Ehepaar Verhindert Schlimmeres 2021. 3 December 2021. Available online: https://www.merkur.de/lokales/muenchen-lk/oberhaching-ort29194/bayern-erste-omikron-faelle-im-landkreis-91154485.html (accessed on 12 December 2022).
- Technologies, B.R.D. Bio-Speedy SARS CoV-2 Double Gene RT-qPCR 2022. Available online: https://www.bioeksen.com.tr/en/biospeedy%C2%AE-sars-cov2-double-gene-rtqpcr (accessed on 12 December 2022).
- Diagnostics, M. ampliCube Coronavirus SARS-CoV-2 2022. Available online: https://www.mikrogen.de/produkte/produktuebersicht/testsystem/coronavirus-panel.html (accessed on 12 December 2022).
- Molbiol, T. SARS Kits and VirSNiP Assays 2022. Available online: https://www.tib-molbiol.de/covid-19 (accessed on 12 December 2022).
- Illumina. Illumina COVIDSeq Test 2022. Available online: https://www.illumina.com/products/by-type/ivd-products/covidseq.html (accessed on 12 December 2022).
- Euronews. Omicron in Europe: Where Have Cases of the New COVID Variant Been Detected? 16 December 2021. Available online: https://www.euronews.com/next/2021/12/13/omicron-in-europe-which-countries-have-detected-cases-of-the-new-covid-variant (accessed on 12 December 2022).
- European Center for Disease Prevention and Control. Epidemiological Update: Omicron Variant of Concern (VOC)—Data as of 30 November 2021 (12.00) 2021 [Updated 30 November 2021]. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-omicron-data-30-november-2021 (accessed on 12 December 2022).
- UK Health Security Agency. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. 10 December 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1042367/technical_briefing-31-10-december-2021.pdf (accessed on 12 December 2022).
- Iuliano, A.D.; Brunkard, J.M.; Boehmer, T.K.; Peterson, E.; Adjei, S.; Binder, A.M.; Cobb, S.; Graff, P.; Hidalgo, P.; Panaggio, M.J.; et al. Trends in Disease Severity and Health Care Utilization During the Early Omicron Variant Period Compared with Previous SARS-CoV-2 High Transmission Periods—United States, December 2020–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Dphil, P.S.B.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Khatib, A.N.; McGuinness, S.; Wilder-Smith, A. COVID-19 transmission and the safety of air travel during the pandemic: A scoping review. Curr. Opin. Infect. Dis. 2021, 34, 415–422. [Google Scholar] [CrossRef]
- Clifford, S.; Quilty, B.J.; Russell, T.W.; Liu, Y.; Chan, Y.-W.D.; Pearson, C.A.B.; Eggo, R.M.; Endo, A.; CMMID COVID-19 Working Group; Flasche, S.; et al. Strategies to reduce the risk of SARS-CoV-2 importation from international travellers: Modelling estimations for the United Kingdom, July 2020. Eurosurveillance 2021, 26, 2001440. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.; Movsisyan, A.; Stratil, J.M.; Biallas, R.L.; Coenen, M.; Emmert-Fees, K.M.; Geffert, K.; Hoffmann, S.; Horstick, O.; Laxy, M.; et al. International travel-related control measures to contain the COVID-19 pandemic: A rapid review. Cochrane Database Syst. Rev. 2021, 3, Cd013717. [Google Scholar]
- Pecoraro, V.; Negro, A.; Pirotti, T.; Trenti, T. Estimate false-negative RT-PCR rates for SARS-CoV-2. A systematic review and meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13706. [Google Scholar] [CrossRef]
- Watson, J.; Whiting, P.F.; Brush, J.E. Interpreting a covid-19 test result. Bmj 2020, 369, m1808. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Buitrago-Garcia, D.; Simancas-Racines, D.; Zambrano-Achig, P.; Del Campo, R.; Ciapponi, A.; Sued, O.; Martinez-García, L.; Rutjes, A.W.; Low, N.; et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE 2020, 15, e0242958. [Google Scholar] [CrossRef]
- Woloshin, S.; Patel, N.; Kesselheim, A.S. False Negative Tests for SARS-CoV-2 Infection—Challenges and Implications. N. Engl. J. Med. 2020, 383, e38. [Google Scholar] [CrossRef]
- Deutsches Bundesgesundheitsministerium [German Federal Ministry of Health]. Verordnung zum Schutz vor Einreisebedingten Infektionsgefahren in Bezug auf das Coronavirus SARS-CoV-2 (Coronavirus-Einreiseverordnung—CoronaEinreiseV) [Regulation on Protection against Entry Related Infection Risks with Regard to the Coronavirus SARS-CoV-2 (Coronavirus Entry Regulation—CoronEinreiseV)]. 2021. Available online: https://www.gesetze-im-internet.de/coronaeinreisev_2021-09/BJNR627200021.html (accessed on 12 December 2022).
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Chapman, A.; Persad, E.; Klerings, I.; Wagner, G.; Siebert, U.; Ledinger, D.; Zachariah, C.; et al. Quarantine alone or in combination with other public health measures to control COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 82, 501–506. [Google Scholar]
- Dickens, B.L.; Koo, J.R.; Lim, J.T.; Sun, H.; Clapham, H.E.; Wilder-Smith, A.; Cook, A.R. Strategies at points of entry to reduce importation risk of COVID-19 cases and reopen travel. J Travel Med. 2020, 27, taaa141. [Google Scholar] [CrossRef] [PubMed]
- Van der Toorn, W.; Oh, D.Y.; Bourquain, D.; Michel, J.; Krause, E.; Nitsche, A.; von Kleist, M. An intra-host SARS-CoV-2 dynamics model to assess testing and quarantine strategies for incoming travelers, contact management, and de-isolation. Patterns 2021, 2, 100262. [Google Scholar] [CrossRef] [PubMed]
- Von Kleist, M.; Ruehe, B.; Oh, D.-J.; Nitsche, A.; Haas, W.; Stoliaroff-Pépin, A.; Eckmanns, T.; Abu Sin, M.; van der Toorn, W.; Jenny, M.; et al. Abwägung der Dauer von Quarantäne und Isolierung bei COVID-19. Zeitschriftenartikel 2020, 39, 3–11. [Google Scholar]

| Characteristics | Total | SARS-CoV-2 Test Result on or within 14 Days after Arrival at Munich Airport | |||
|---|---|---|---|---|---|
| Positive on Arrival | Negative on Arrival but Positive within 14 Days after Arrival | Negative on Arrival and Did Not Become Positive within 14 Days after Arrival | Negative on Arrival and No Information on Infection within 14 Days after Arrival † | ||
| N = 528 (100%) | n = 26 (4.9%) | n = 21 (4.2%) | n = 469 (89%) | n = 12 (2.3%) | |
| Role during flight | |||||
| Passenger | 452 (92%) | 25 (100%) | 20 (100%) | 405 (91%) | 2 (100%) |
| Crew | 41 (8.3%) | 0 (0%) | 0 (0%) | 41 (9.2%) | 0 (0%) |
| Age in years (median [IQR]) | |||||
| 49 [36–60] | |||||
| 6–18 | 8 (1.6%) | 1 (3.8%) | 1 (4.8%) | 6 (1.3%) | 0 (0%) |
| 19–34 | 113 (22%) | 14 (54%) | 13 (62%) | 231 (49%) | 1 (33%) |
| 35–64 | 318 (62%) | 9 (35%) | 6 (29%) | 156 (33%) | 1 (33%) |
| ≥65 | 78 (15%) | 2 (7.7%) | 1 (4.8%) | 74 (16%) | 1 (33%) |
| Gender | |||||
| Male | 272 (53%) | 14 (54%) | 5 (24%) | 251 (54%) | 2 (67%) |
| Female | 245 (47%) | 12 (46%) | 16 (76%) | 216 (46%) | 1 (33%) |
| Diverse | 1 (0.2%) | 0 (0%) | 0 (0%) | 1 (0.2%) | 0 (0%) |
| SARS-CoV-2 variant, for those testing positive on or within 14 days after arrival (n = 47) | |||||
| Omicron | 37 (80%) | 21 (81%) | 16 (80%) | n.a. | n.a. |
| Delta | 3 (6.5%) | 1 (3.8%) | 2 (10%) | n.a. | n.a. |
| Unknown | 6 (13%) | 4 (15%) | 2 (10%) | n.a. | n.a. |
| Any other travelers in the travel group tested positive for SARS-CoV-2 | |||||
| Yes | 60 (13%) | 7 (30%) | 9 (45%) | 44 (10%) | 0 (0%) |
| No | 321 (67%) | 11 (48%) | 8 (40%) | 301 (70%) | 1 (100%) |
| Unknown | 95 (20%) | 5 (22%) | 3 (15%) | 87 (20%) | 0 (0%) |
| Close contact in South Africa with a person who subsequently tested positive for SARS-CoV-2 | |||||
| Yes | 72 (15%) | 5 (21%) | 3 (15%) | 64 (15%) | 0 (0%) |
| No | 318 (66%) | 15 (62%) | 15 (75%) | 288 (66%) | 0 (0%) |
| Unknown | 92 (19%) | 4 (17%) | 2 (10%) | 85 (19%) | 1 (100%) |
| Any underlying chronic condition | |||||
| Yes | 29 (15%) | 7 (27%) | 3 (14%) | 3 (0.6%) | 0 (0%) |
| No | 433 (84%) | 19 (73%) | 18 (86%) | 395 (85%) | 1 (100%) |
| Unknown | 3 (0.6%) | 0 (0%) | 0 (0%) | 3 (0.6%) | 0 (0%) |
| Regulation or Measure # | Total | SARS-CoV-2 Test Result on or within 14 Days after Arrival at Munich Airport | |||
|---|---|---|---|---|---|
| Positive on Arrival | Negative on Arrival but Positive within 14 Days after Arrival | Negative on Arrival and Did Not Become Positive within 14 Days after Arrival | Negative on Arrival and No Information on Infection within 14 Days after Arrival Available | ||
| N = 528 (100%) | n = 26 (4.9%) | n = 21 (4%) | n = 469 (89%) | n = 12 (2%) | |
| Vaccination status † | |||||
| Fully vaccinated | 405 (77%) | 22 (85%) | 18 (86%) | 364 (78%) | 1 (8.3%) |
| Not fully vaccinated | 62 (12%) | 1 (3.8%) | 3 (14%) | 57 (12%) | 1 (8.3%) |
| Not vaccinated | 19 (3.6%) | 1 (3.8%) | 0 (0%) | 18 (3.8%) | 0 (0%) |
| Type of mask worn during flight | |||||
| FFP2 (KN95) mask or multiple mask types, including FFP2 | 383 (80%) | 21 (88%) | 18 (90%) | 343 (79%) | 1 (100%) |
| Only medical mask | 91 (19%) | 3 (12%) | 2 (10%) | 86 (20%) | 0 (0%) |
| Fabric mask or no mask | 7 (1.5%) | 0 (0%) | 0 (0%) | 7 (1.6%) | 0 (0%) |
| Negative SARS-CoV-2 test result before departure | |||||
| Yes, PCR test | 392 (74%) | 19 (86%) | 17 (89%) | 355 (84%) | 1 (100%) |
| <12 h old | 19 (4.1%) | 0 (0%) | 0 (0%) | 19 (4.5%) | 0 (0%) |
| ≥12 to <24 h old | 159 (34%) | 6 (27%) | 7 (37%) | 146 (34%) | 0 (0%) |
| ≥24 to <48 h old | 211 (45%) | 13 (59%) | 10 (53%) | 187 (44%) | 1 (100%) |
| Unknown period of time | 3 (0.64%) | 0 (0%) | 0 (0%) | 3 (0.7%) | 0 (0%) |
| Yes, antigen test | 22 (4.7%) | 2 (9.1%) | 1 (5.3%) | 19 (4.5%) | 0 (0%) |
| <12 h old | 9 (2%) | 0 (0%) | 0 (0%) | 9 (2.1%) | 0 (0%) |
| ≥12 to <24 h old | 9 (2%) | 2 (9.1%) | 1 (5.3%) | 6 (1.4%) | 0 (0%) |
| ≥24 to <48 h old | 3 (0.64%) | 0 (0%) | 0 (0%) | 3 (0.7%) | 0 (0%) |
| Unknown period of time | 1 (0.21%) | 0 (0%) | 0 (0%) | 1 (0.24%) | 0 (0%) |
| Yes, but unknown type | 1 (0.2%) | 0 (0%) | 0 (0%) | 1 (0.2%) | 0 (0%) |
| No test | 48 (10%) | 1 (4.5%) | 0 (0%) | 47 (11%) | 0 (0%) |
| Unknown | 4 (0.9%) | 0 (0%) | 1 (5.3%) | 3 (0.7%) | 0 (0%) |
| Quarantine/Isolation after arrival | |||||
| Yes | 393 (80%) | 26 (100%) | 21 (100%) | 372 (80%) | 1 (100%) |
| No | 96 (20%) | 0 | 0 | 95 (20%) | 0 (0%) |
| Fulfilled entry regulations § | |||||
| Yes | 360 (76%) | 21 (96%) | 17 (94%) | 321 (74%) | 1 (100%) |
| No | 116 (24%) | 1 (4.5%) | 1 (5.5%) | 114 (26%) | 0 |
| Total | Tested Positive for SARS-CoV-2 on Arrival at Munich Airport | Univariable Analysis | |||
|---|---|---|---|---|---|
| Characteristics | Yes | No | RR (95% CI) | p-Value | |
| N = 528 (100%) | n = 26 (4.9%) | n = 502 (95%) | |||
| Age, years | |||||
| >34 | 121 (23%) | 7 (6%) | 114 (94%) | Ref. | |
| ≤35 | 396 (77%) | 19 (5%) | 377 (95%) | 0.83 (0.37–2.08) | 0.66 |
| Gender | |||||
| Male | 272 (53%) | 14 (5%) | 258 (95%) | Ref. | |
| Female | 245 (47%) | 12 (5%) | 233 (95%) | 0.95 (0.44–2.02) | 0.90 |
| Diverse | 1 (0.2%) | 0 (0%) | 1 (100%) | Omitted | |
| Vaccination status † | |||||
| Not (fully) vaccinated | 81 (17%) | 2 (2.5%) | 79 (97.5%) | Ref. | |
| Fully vaccinated | 405 (83%) | 22 (5%) | 383 (95%) | 2.20 (0.67–13.6) | 0.28 |
| Previous SARS-CoV-2 infection | |||||
| No/unknown | 437 (87%) | 22 (5%) | 415 (95%) | Ref. | |
| Yes | 65 (13%) | 3 (5%) | 62 (95%) | 0.92 (0.22–2.55) | 0.89 |
| Negative SARS-CoV-2 test result before departure | |||||
| No/unknown | 52 (11%) | 1 (2%) | 51 (98%) | Ref. | |
| Yes | 415 (89%) | 21 (5%) | 349 (95%) | 2.63 (0.57–46.7) | 0.34 |
| Time between any negative test and departure | |||||
| ≥24 to <48 h | 211 (46%) | 13 (6.2%) | 198 (94%) | Ref. | |
| < 24 h | 199 (43%) | 8 (4.0%) | 191 (96%) | 0.65 (0.26–1.51) | 0.33 |
| No test | 48 (10%) | 1 (2.1%) | 47 (98%) | Omitted | |
| Travel partner tested positive for SARS-CoV-2 | |||||
| No/unknown | 416 (87%) | 16 (4%) | 400 (96%) | Ref. | |
| Yes | 60 (13%) | 7 (12%) | 53 (88%) | 3.03 (1.21–6.80) | 0.010 |
| Close contact in South Africa with a person who subsequently tested positive for SARS-CoV-2 | |||||
| No/unknown | 410 (85%) | 19 (5%) | 391 (95%) | Ref. | |
| Yes | 72 (15%) | 5 (7%) | 67 (93%) | 1.50 (0.51–3.59) | 0.41 |
| Kept at least a 1.5 m distance | |||||
| Never/rarely | 47 (10%) | 1 (2%) | 46 (98%) | Ref. | |
| Sometimes | 52 (11%) | 3 (6%) | 49 (94%) | 2.48 (0.54–44.0) | 0.37 |
| Always/often | 379 (79%) | 20 (5%) | 359 (95%) | 2.71 (0.36–53.8) | 0.38 |
| Disinfected hands several times per day | |||||
| Never/rarely | 52 (11%) | 1 (2%) | 51 (98%) | Ref. | |
| Sometimes | 61 (13%) | 3 (5%) | 58 (95%) | 2.56 (0.34–50.9) | 0.41 |
| Always/often | 366 (76%) | 20 (5%) | 346 (95%) | 2.84 (0.61–50.5) | 0.30 |
| Washed hands several times per day | |||||
| Never/rarely | 19 (4%) | 2 (11%) | 17 (89%) | Ref. | |
| Sometimes | 62 (13%) | 1 (2%) | 61 (98%) | 0.15 (0.01–1.52) | 0.12 |
| Always/often | 398 (83%) | 21 (5%) | 377 (95%) | 0.50 (0.16–2.99) | 0.33 |
| Wore FFP2 mask | |||||
| Never/rarely | 128 (27%) | 6 (5%) | 122 (95%) | Ref. | |
| Sometimes | 65 (14%) | 6 (9%) | 59 (91%) | 1.97 (0.64–6.07) | 0.22 |
| Always/often | 281 (59%) | 12 (4%) | 269 (96%) | 0.91 (0.36–2.57) | 0.85 |
| Wore medical mouth-nose mask | |||||
| Never/rarely | 192 (44%) | 11 (6%) | 181 (94%) | Ref. | |
| Sometimes | 58 (13%) | 4 (7%) | 54 (93%) | 1.20 (0.34–3.37) | 0.74 |
| Always/often | 190 (43%) | 9 (5%) | 181 (95%) | 0.83 (0.34–1.95) | 0.66 |
| Wore fabric mask | |||||
| Never/rarely | 367 (86%) | 18 (5%) | 349 (95%) | Ref. | |
| Sometimes | 16 (4%) | 1 (6%) | 15 (94%) | 1.27 (0.07–5.59) | 0.81 |
| Always/often | 43 (10%) | 5 (12%) | 38 (88%) | 2.37 (0.82–5.61) | 0.072 |
| Wore mask only indoors | |||||
| Never/rarely | 31 (6%) | 0 (0%) | 31 (100%) | Omitted | |
| Sometimes | 50 (11%) | 3 (6%) | 47 (94%) | Ref. | |
| Always/often | 392 (83%) | 21 (5%) | 371 (95%) | 0.89 (0.32–3.69) | 0.85 |
| Wore mask indoors and outdoors | |||||
| Never/rarely | 250 (54%) | 7 (3%) | 243 (97%) | Ref. | |
| Sometimes | 107 (23%) | 7 (7%) | 100 (93%) | 2.34 (0.82–6.67) | 0.10 |
| Always/often | 109 (23%) | 10 (9%) | 99 (91%) | 3.28 (1.29–8.81) | 0.013 |
| Avoided contact with people outside my travel group | |||||
| Never/rarely | 165 (35%) | 3 (2%) | 162 (98%) | Ref. | |
| Sometimes | 150 (31%) | 12 (8%) | 138 (92%) | 4.40 (1.43–19.1) | 0.020 |
| Always/often | 162 (34%) | 9 (6%) | 153 (94%) | 3.06 (0.93–13.6) | 0.089 |
| Avoided mass transportation | |||||
| Never/rarely | 413 (87%) | 17 (4%) | 396 (96%) | Ref. | |
| Sometimes | 38 (8%) | 2 (5%) | 36 (95%) | 1.26 (0.18–6.20) | 0.78 |
| Always/often | 26 (5%) | 5 (19%) | 21 (81%) | 4.62 (1.31–17.6) | 0.016 |
| Avoided crowds | |||||
| Never/rarely | 194 (41%) | 8 (4%) | 186 (96%) | Ref | |
| Sometimes | 145 (31%) | 11 (8%) | 134 (92%) | 1.84 (0.76–4.64) | 0.18 |
| Always/often | 135 (28%) | 5 (4%) | 130 (96%) | 0.90 (0.28–2.63) | 0.85 |
| Characteristics | Total | Tested Positive for SARS-CoV-2 within 14 Days after Arrival | Univariable Analysis | ||
|---|---|---|---|---|---|
| Yes | No | RR (95% CI) | p-Value | ||
| N = 490 (100%) | n = 21 (4%) | n = 469 (96%) | |||
| Role in airplane | |||||
| Crew | 41 (8.8%) | 0 (%) | 41 (100%) | Omitted | |
| Passenger | 427 (91%) | 20 (5%) | 405 (95%) | ||
| Age, years | |||||
| ≤34 | 113 (23%) | 9 (8%) | 104 (92%) | Ref. | |
| ≥35 | 375 (77%) | 12 (3%) | 363 (97%) | 0.40 (0.17–0.96) | 0.033 |
| Gender | |||||
| Male | 256 (52%) | 5 (2%) | 251 (98%) | Ref. | |
| Female | 232 (47%) | 16 (7%) | 216 (93%) | 3.53 (1.41–10.7) | 0.012 |
| Diverse | 1 (1%) | 0 (0%) | 1 (100%) | Omitted | |
| Vaccination status † | |||||
| Not (fully) vaccinated | 78 (17%) | 3 (4%) | 75 (96%) | Ref. | |
| Fully vaccinated | 382 (83%) | 18 (5%) | 364 (95%) | 1.23 (0.43–5.14) | 0.74 |
| Previous SARS-CoV-2 infection | |||||
| No/unknown | 414 (87%) | 19 (5%) | 395 (95%) | Ref. | |
| Yes | 62 (13%) | 1 (2%) | 61 (98%) | 0.35 (0.02–1.65) | 0.304 |
| Fulfilled entry regulations § | |||||
| No | 115 (25%) | 1 (1%) | 114 (99%) | Ref. | |
| Yes | 338 (75%) | 17 (5%) | 321 (95%) | 5.78 (1.21–104) | 0.086 |
| Type of mask worn during flight | |||||
| Wore FFP2 (KN95) (vs not) | 361 (79%) | 18 (5%) | 343 (95%) | 2.37 (0.70–14.7) | 0.24 |
| Wore medical mouth-nose mask (vs not) | 88 (19%) | 2 (2%) | 86 (98%) | 0.47 (0.075–1.57 | 0.30 |
| Wore mask continuously | |||||
| No, not always | 401 (88%) | 18 (4%) | 383 (96%) | Ref. | |
| Yes, during entire flight | 55 (12%) | 2 (4%) | 53 (96%) | 0.81 (0.13–2.70) | 0.77 |
| Consumed food | |||||
| No or once | 92 (20%) | 4 (4%) | 88 (96%) | Ref. | |
| Several times | 361 (80%) | 16 (4%) | 345 (96%) | 1.02 (0.38–3.49) | 0.97 |
| Consumed drinks | |||||
| No or once | 30 (7%) | 2 (6%) | 28 (93%) | Ref. | |
| Several times | 425 (93%) | 18 (4%) | 407 (96%) | 0.64 (0.20–3.88) | 0.53 |
| Visited toilet | |||||
| No or once | 96 (21%) | 3 (3%) | 93 (97%) | Ref. | |
| Several times | 358 (79%) | 17 (5%) | 341 (95%) | 1.52 (0.52–6.41) | 0.50 |
| Conversation with people in close proximity (within 2 m) | |||||
| No or once | 235 (52%) | 14 (6%) | 221 (94%) | Ref. | |
| Several times | 217 (48%) | 6 (3%) | 211 (97%) | 0.46 (0.17–1.13) | 0.13 |
| Travel partner tested positive for SARS-CoV-2 | |||||
| No/unknown | 399 (88%) | 11 (3%) | 388 (97%) | Ref. | |
| Yes | 53 (12%) | 9 (17%) | 44 (83%) | 6.16 (2.60–14.2) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidl, C.; Coyer, L.; Ackermann, N.; Katz, K.; Walter, J.; Ippisch, S.; Hoch, M.; Böhmer, M.M. SARS-CoV-2 Prevalence on and Incidence after Arrival in Travelers on Direct Flights from Cape Town, South Africa to Munich, Germany Shortly after Occurrence of the Omicron Variant in November/December 2021: Results from the OMTRAIR Study. Pathogens 2023, 12, 354. https://doi.org/10.3390/pathogens12020354
Seidl C, Coyer L, Ackermann N, Katz K, Walter J, Ippisch S, Hoch M, Böhmer MM. SARS-CoV-2 Prevalence on and Incidence after Arrival in Travelers on Direct Flights from Cape Town, South Africa to Munich, Germany Shortly after Occurrence of the Omicron Variant in November/December 2021: Results from the OMTRAIR Study. Pathogens. 2023; 12(2):354. https://doi.org/10.3390/pathogens12020354
Chicago/Turabian StyleSeidl, Cornelia, Liza Coyer, Nikolaus Ackermann, Katharina Katz, Jan Walter, Siegfried Ippisch, Martin Hoch, and Merle M. Böhmer. 2023. "SARS-CoV-2 Prevalence on and Incidence after Arrival in Travelers on Direct Flights from Cape Town, South Africa to Munich, Germany Shortly after Occurrence of the Omicron Variant in November/December 2021: Results from the OMTRAIR Study" Pathogens 12, no. 2: 354. https://doi.org/10.3390/pathogens12020354